After completing my history of rural electrification in the United States, I began work on a seemingly unrelated topic—a history of techniques and technologies used to resuscitate victims of electric shock and drowning. The choice of the topic seems, on the surface, to make little sense. After all, for more than 40 years, I had been writing about the electric utility system, dealing with the history of power companies’ management, culture, technological choices, regulation, deregulation, and the increasing emphasis, in the twenty-first century, of energy-efficiency techniques and renewable energy. What does any of this past work have to do with the development of things like automatic external defibrillators (AEDs) and cardiopulmonary resuscitation (CPR)?
Actually, quite a bit. Let me tell you how.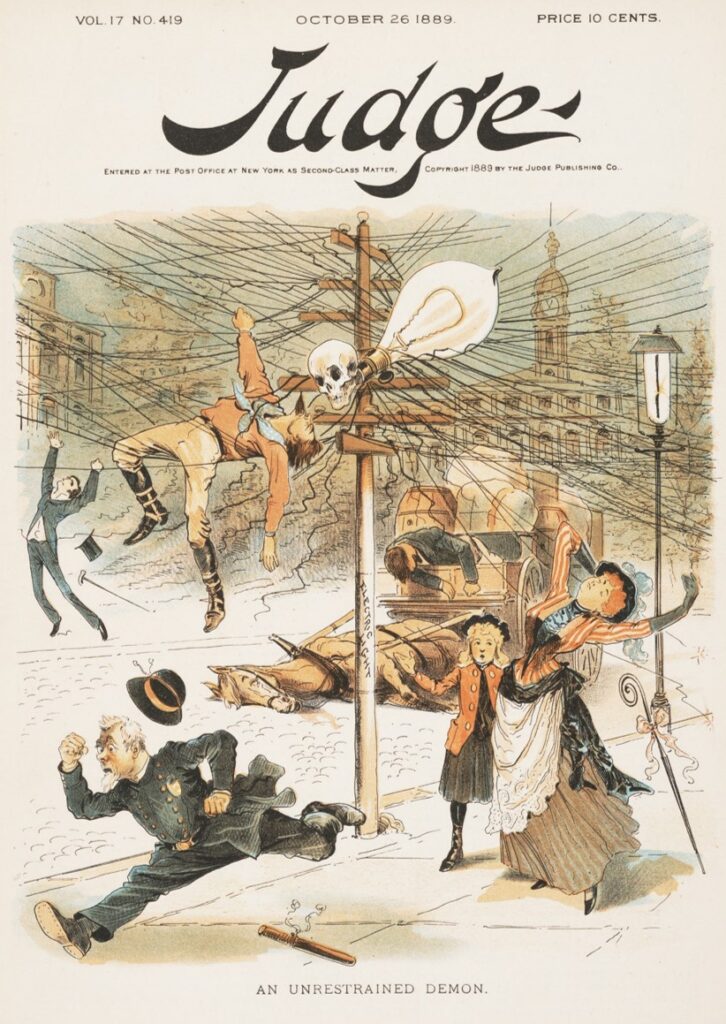
It turns out that the emerging electric utility industry in the 1880s encountered a serious practical and public-relations problem. In particular, too many of its workers and customers died from electrical shocks. Linemen and power plant operators often inadvertently contacted high-current cables, while customers sometimes died after touching inadequately insulated wires or poorly grounded appliances. In one gruesome event covered by sensationalist newspapers and magazines, lineman John Feeks died “in agony before the eyes of thousands” after touching an unexpectedly charged wire above the streets of New York City on 11 October in 1889. Onlookers gasped as they saw “the unfortunate fellow’s mouth and nostrils belch[ing] forth white smoke. He was literally roasting to death.” Luridly, the newspaper reported that “[a] more thrilling sight, it is safe to say, was never seen in New York.” [1] The next day’s paper observed that the lineman’s pregnant wife was “very low” and grieving in bed while knowing that his unborn child “will never know the father.”[2] So tragic and so apparently common was this type of accident that the city’s mayor threatened to act against electric companies.[3]
Such public exhibitions of the dangerous nature of electricity could not have been good news to the managers of the many newly created power companies populating New York and other American cities. After all, the leaders of the hundreds of electric companies in the US tried to capitalize on the sense of awe that, as historian David Nye has nicely expressed, most people felt when they saw electric light bulbs for the first time.[4] But as accidents such as Feeks’ demonstrated, electricity also was something to fear. To add to this public sense of wariness about electricity, supporters of Thomas Edison’s direct current electricity systems had escalated a “war of the currents” in 1888 with publications about the dangerous nature of alternating current systems, advanced by George Westinghouse. Well covered stories in newspapers detailed public demonstrations of the use of electricity to kill animals, with the New York State legislature passing a bill (signed by the governor on 4 June 1888)) to use electricity for electrocution of criminals. (The first was executed on 6 August 1890.)[5]
To deal with such “image” problems, the industry, through its trade organization, the National Electric Light Association (NELA, founded in 1885), worked to establish standards and best practices to eliminate the possibility of electrocutions, with some success. As early as 1894, electric company managers showed interest in applying these resuscitation principles to those who suffered apparent death from electrocution. In articles published in Electrical World, the industry’s main trade journal, one could read about the supposed physiological causes of death from electrocution[6] and methods to revive shocked victims.[7] The journal also produced an easy-to-use instruction sheet (with illustrations) for distribution to electric company employees.[8]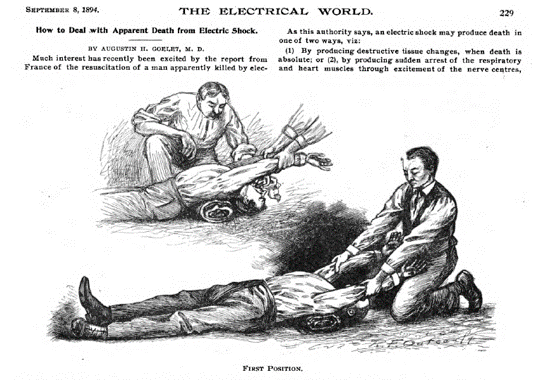
The industry took a more concerted effort in 1912, when NELA created a “Resuscitation Commission,” which sought to increase the welfare of power company employees. Members of the group included reputable physicians and utility representatives.[9] representing the American Medical Association, professors from Harvard and elsewhere, Elihu Thomson (one of the founders of General Electric),[10] and Arthur E Kennelly of Harvard. Individual companies also appeared to be interested in developing effective techniques to save electrocuted workers. New York’s Consolidated Edison Company of New York (ConEd), for example, worked with medical organizations and funded the Johns Hopkins School of Hygiene and Public Health to work toward understanding how to resuscitate electrocuted victims. Interestingly, the Hopkins team included principal investigator, neurologist Orthello Langworthy, who invited a professor of electrical engineering, William Kouwenhoven, to join his funded group. Together (and with others, along with later funding from the Edison Electric Institute, the successor organization to NELA), the group worked through the 1960s and developed a clearer understanding of cardiac fibrillation, a frequent cause of death. More significantly, perhaps, the group invented devices (defibrillators) to reverse the condition without surgical intervention. By accident, the group also discovered it could replicate the heart’s pumping action by performing compressions on a patient’s chest. In a landmark 1960 article, the team described the basis of modern CPR, noting that “[a]nyone, anywhere, can now initiate cardiac resuscitative procedures. All that is needed are two hands.”[11]
In short, the utility industry played a fairly significant role in the development of techniques used to save lives of people having heart attacks. That connection explains perhaps HALF of my interest in this topic.
The other half comes from my passion for emergency medicine. Even while working as a traditional university academic, I have served for more than three decades as a volunteer emergency medical technician (EMT). Trained and certified in the Commonwealth of Virginia, I work with the Virginia Tech Rescue Squad, an unusual (but highly skilled and professional) organization that has been managed by student members for more than 55 years. (It remains the oldest student-run rescue squad in the United States.) The squad contains three non-students, with me being one of them. Also certified as a CPR provider (and instructor), I’ve enjoyed learning about resuscitative techniques and have been aware of changes and improvements in them over the years.
My discovery that the electric utility industry contributed to the creation of some of the approaches I use as an EMT motivated me to combine my academic and volunteer interests. This project on the history of resuscitative techniques and technologies, which began in 2022, is the result.
While my primary focus concerns the history of approaches to revive victims of cardiac problems, I also investigate and draw upon the history of techniques to save those who had apparently drowned and died. This line of research has merit for at least two reasons. First, some of the techniques that earlier gained favor for drowning victims were adopted by utility industry managers. After all, if people knew how to revive those who had drowned—having no heartbeat in many instances and having stopped breathing—then the same approaches should logically apply to those who apparently died from electric shocks. Secondly, an investigation into the history of resuscitation techniques for drowning patients provides a lens through which one can look at the contingent nature of understanding about medical knowledge. As will be noted below, some of the techniques that seemed to work well, and which appeared to have been well documented, appear laughable today.
The history of formal efforts to understand and popularize resuscitation techniques for drowning victims dates to the creation in 1767 of the Society for the Recovery of Drowned Persons in Amsterdam and its counterpart in London, England, the Royal Humane Society, established in 1774. The latter organization published accounts of people who claimed to have saved the lives of drowning victims. Physicians and scientists employed these reports and other evidence to develop what appeared to be useful guidelines and techniques to standardize resuscitative techniques. They also hoped to make them simple enough for everyday people and laborers in various fields (such as water-borne and mining industries) to exploit, thus saving (or potentially saving) hundreds of lives yearly.
Closer examination of these accounts, however, suggests skepticism about the supposed successes and progress. A modern observer—even one without formal medical training—would question whether blowing tobacco smoke “or some aromatic herb, as sage, mint or rosemary” into the anus of a nonbreathing drowning victim really had positive effects.[12] 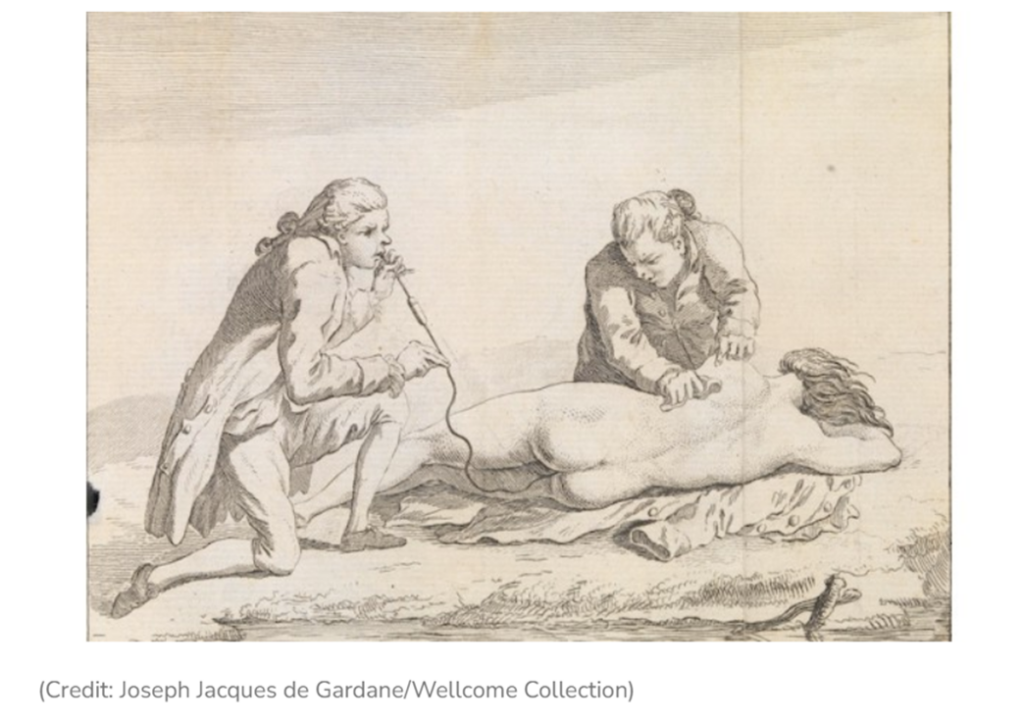 Likewise, did the application of static electricity twenty minutes after apparent death really restore life to a child who had fallen from a window in 1774?[13] Overall, the Humane Society reported that between 1774 and 1793, 959 successful cases of resuscitation occurred (out of 1,706—a 56.2 percent success rate) using techniques that would largely be discredited today.[14] While some of these approaches lost favor over the years, others (such as the “prone pressure” technique) gained widespread acceptance and use.[15]
Likewise, did the application of static electricity twenty minutes after apparent death really restore life to a child who had fallen from a window in 1774?[13] Overall, the Humane Society reported that between 1774 and 1793, 959 successful cases of resuscitation occurred (out of 1,706—a 56.2 percent success rate) using techniques that would largely be discredited today.[14] While some of these approaches lost favor over the years, others (such as the “prone pressure” technique) gained widespread acceptance and use.[15]
An examination of the history of resuscitation provides insight into the nature of knowledge and evidence in the realm of medicine. On one hand, historians (and others) view modernity as characterized in part by the development and use of theories, techniques, and technologies based on empirical evidence and experimentation. On the other hand, as historians of science and technology have noted for decades, the social context, beliefs, assumptions, and cultures of practitioners influence their choices of research questions and interpretations of experimental results.
Aside from documenting a history of techniques and technologies to revive the apparently dead, I’m therefore investigating the epistemology of resuscitative medicine—how did people develop “knowledge” about saving people who appeared to have died? While we may look back and be amused (or horrified) by some of the “knowledge” acquired by earlier practitioners, we need to remain humble about our own state of affairs—a point I seek to make as we explore the past for lessons that have value today. After all, our modern resuscitative methods, supposedly based on good evidence and scientific knowledge, still remain ineffective on the vast majority of patients. In fact, only about 10 percent of people who receive out-of-hospital care for cardiac arrests survive and return to normal lives.[16] That percentage is better than having no chance at having life restored, but it means that we have not yet mastered the means to cheat the Grim Reaper frequently enough.
Notes
[1] “On a Live Wire,” New York Evening World, 11 October 1889, 1. Newspapers.com thru lib.vt.edu.
[2] “All Aroused,” New York Evening World, 12 October 1889, 1.
[3] The city had seen at least nine electrocution deaths since the beginning of 1887. “An Alarming Record,” New York Evening World, 12, October 1889, 1. Newspapers reported similar fatalities in the years before, in New York and elsewhere. Examples: “Killed by An Electric Shock: Instantaneously Fatal Result of a Current from a Brush-Light Machine,” New York Times, 11 August 1881, 5, reporting on an event in Buffalo, NY; “Killed by an Electric Shock: Tragic Death of a Workman While Changing Electric Light Wires,” New York Times, 5 October 1882, 8; and “Killed by an Electric Shock,” New York Times, 30 December 1885, 1, reporting on an “Italian organ Grinder” who died when touching a drooping electric wire in New Orleans.
[4] The use of electric lights to inspire awe is explored in David E. Nye, American Technological Sublime (Cambridge, MA: MIT Press, 1994), 143-72.
[5] Terry S. Reynolds and Theodore Bernstein, “Edison and ‘The Chair,’” IEEE Technology and Society Magazine 8 no. 1 (March 1989): 21 and 24 (article runs 19-28).
[6] “Does Electricity Kill?,” Electrical World 24, no. 2 (14 July 1894): 23-24.
[7] Augustin H. Goelet, M.D. “How to Deal with Apparent Death from Electric Shock,” Electrical World 24, no. 10 (8 Sept. 1894): 229-31.
[8] An editorial noted that the journal published “a detailed account of the treatment to which a patient should be subjected.” “Resuscitation from Electric Shocks,” editorial in Electrical World 54, no. 10 (8 September 1894): 228.
[9] Address of President [John F.] Gilchrist,” NELA, 35th convention, volume 1, June 10-23, 1912, pp. 18-19. “Report of Committee on Resuscitation from Electrical Shock,” report in the 1912 issue. Fuller report of the commission’s makeup and work appeared in Commission on Resuscitation from Electric Shock” was printed in the 1913 issue of the NELA convention (36th convention, Chicago, June 2-6, 1913, pp. 324-345).
[10] Thomson may have been motivated to serve on this committee because of his concerns for safety, which he expressed in 1887 and later, when his company shipped its first AC machines. See W. Bernie Carlson, Innovation as a Social Process: Elihu Thomson and the Rise of General Electric (New York: Cambridge University Press, 1991), 259. Thomson realized that some utilities, eager to sell electricity and make a return on investments, often failed to use sufficiently effective insulators, “and their linemen often were careless and indifferent to the special requirements of alternating current.” (Ibid., 260).
[11] W. B. Kouwenhoven, James R. Jude, and G. Guy Knickerbocker, “Closed-Chest Cardiac Massage,” JAMA 173, (9 July 1960): 1064.
[12] Alexander Johnson, M.D., Summary Instructions For the general Institution, proposed in the Year 1773, to Introduce and Establish, In his Majesty’s British Dominions, A Successful Practice for Recovering Person who meet with Accidents Producing Suddenly an Appearance of Death, and Preventing their being buried alive (London: T. Hodgson, 1773 and 1785), 12. Also cited in Cary, 1913, p. 243.
[13] W. Hawes, M.D., Transactions of the Royal Humane Society from 1774 to 1784, vol. 1 (London: Jno. Nichols, 1795), 51.
[14] The techniques included “fumigation,” which consists of filling the great bowel with tobacco smoke. Arthur Keith, MD, “Lecture III—the Period of Mechanical Movements of the Chest Wall,” part of “Three Hunterian Lectures on the Mechanism Underlying the Various Methods of Artificial Respiration Practiced Since the Foundation of the Royal Humane Society in 1774,” Lancet 173, issue 4465 (27 March 1909): 897. From Keith, March 13, 1909: Arthur Keith, M.D. “Lecture 1,” Lancet 170, issue 4463 (13 March 1909): 746.
[15] Into the early 20th century, the Silvester and Schafer “prone pressure” technique became the most widely used, with supposedly good data supporting its use. E.A. Schafer, FRS, “Artificial Respiration in its Physiologic Aspects,” Journal of the American Medical Association 51, no. 10 (5 September 1908): 801-803.
[16] Cardiac Arrest Registry to Enhance Survival (CARES), 2023 Annual Report: Data Highlights, Successes, and Future Directions at https://mycares.net.